When Normal Science fails: a clinical anomaly that opens the problem 1
__NOTITLE__
When Normal Science Fails: a clinical anomaly that opens the problem
 |
Introduction
This chapter opens the section dedicated to the Index. It does not yet introduce the Index in its operational formulation, but it builds its clinical and epistemological rationale.
The starting point is not theoretical, but clinical: a set of findings that, while formally correct according to the standard diagnostic models currently in use, have proven over time insufficient to provide an adequate understanding of the complexity of the observed clinical pictures. Epidemiological studies based on RDC/TMD and DC/TMD criteria[1] indeed show a high prevalence of temporomandibular disorders in the general population—estimated at close to 30%—while also highlighting that these conditions represent a widely underestimated health burden and are not yet fully understood at the clinical level.
Consistently with this picture, recent studies on the use of large language models as diagnostic support in orofacial pain show that, even in the presence of high formal accuracy with respect to standard criteria, significant difficulties remain in discriminating overlapping clinical pictures and in managing complex symptom contexts.[2]
What emerges, therefore, is not a simple classification error, but a deeper difficulty in coherently linking signs, symptoms, and functional dynamics within a single interpretive framework. This difficulty signals the possible structural limit of a predominantly descriptive diagnostic paradigm, grounded in discrete categories, classical probabilities, and the implicit assumption that clinical information can be treated as stable and independent of the context of observation.
A non-eliminable clinical anomaly
In the Normal Science section, a prospective study conducted on 40 subjects was presented, including 30 asymptomatic and 10 symptomatic individuals. By applying the RDC (Research Diagnostic Criteria), a substantial proportion of symptomatic subjects was classified as having temporomandibular disorders (TMD).
However, the clinical follow-up years later revealed that a significant portion of these patients actually had severe neurological and systemic diseases (meningiomas, pineal cavernomas, scleroderma, hemimasticatory spasm). In some cases, diagnostic delay entailed a concrete risk to the patient’s life.
These findings cannot be dismissed as simple “false positives.”
They constitute an epistemological anomaly:Consistently with this observation, independent studies comparing clinical diagnosis based on RDC/TMD criteria with high-resolution imaging techniques have shown low agreement and a marked reduction in diagnostic sensitivity, indicating that a substantial fraction of structural alterations of the temporomandibular system remains clinically invisible when observed exclusively through standard descriptive criteria.[3] In parallel, the rigorous application of DC/TMD imaging criteria on high-resolution CBCT has shown a high frequency of degenerative findings even in asymptomatic subjects, suggesting a systematic discrepancy between structural description and the clinical state of the system.[4]the model produces local certainties that do not coincide with the global clinical reality of the system.
The problem is not a lack of data
TMD, orofacial pain, and masticatory functions in general are among the most studied conditions in dentistry and neurology. Many works have documented the multifactorial nature of these disorders, the interaction between peripheral and central factors, and the high overlap with other pathological conditions.
Yet, despite the abundance of data, diagnostic difficulties persist.
This indicates that the problem does not lie in the amount of information available, but in the way such information is organized, interpreted, and integrated within the diagnostic process.[5]When a condition is defined as “multifactorial” and managed only ex post through multimodal strategies, this implies that ex ante there is no integrated diagnostic criterion capable of coherently guiding clinical decision-making.
Probabilistic certainty and clinical truth
By applying the RDC model to the data from the prospective study and using Bayes’ theorem, it is possible to obtain an extremely high conditional probability:
Within the model, this certainty is formally correct. However, follow-up shows that such certainty does not necessarily coincide with clinical truth: a “certain” diagnosis may coexist with a severe pathology not detected by the model.
An emblematic example is represented by patients initially classified as having TMD according to RDC criteria—sometimes framed as bruxists—in whom follow-up later revealed the presence of structural neurological pathologies, such as pineal cavernomas. In these cases, the probabilistically “certain” diagnosis temporarily masked a clinical picture of a radically different nature.-
 Figure 1: MRI images of the temporomandibular joint (right side shown only for simplification) show no signs of disc displacement and/or inflammation. Report negative.
Figure 1: MRI images of the temporomandibular joint (right side shown only for simplification) show no signs of disc displacement and/or inflammation. Report negative. -
 Figure 2: Axiographic tracing performed with a paraocclusal tray showing a normal translatory and mediotrusive pattern of the right condyle. Report negative.
Figure 2: Axiographic tracing performed with a paraocclusal tray showing a normal translatory and mediotrusive pattern of the right condyle. Report negative. -
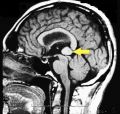 Figure 3: On the sagittal plane of contrast-enhanced brain MRI (gadolinium), an extensive cavernoma is visible (arrow).
Figure 3: On the sagittal plane of contrast-enhanced brain MRI (gadolinium), an extensive cavernoma is visible (arrow).



high statistical probability ≠ clinical truth. The discrepancy does not concern a calculation error, but the model’s domain of validity.
The role of time and observational order
One element emerges clearly from longitudinal data: time is not an accessory variable, but a structuring dimension of diagnosis.
The order in which tests are performed determines which aspects of the biological system become observable and which remain latent. It follows that diagnosis is not only a function of “which data” are collected, but also of “when” and “in what sequence” they are observed.
This breaks an implicit assumption of classical models: the commutativity of clinical information.
Informational non-commutativity (clinical reading)
If two diagnostic tests are represented as informational operators and , the result of observation may depend on the order of application:
In clinical terms, performing first a test with low sensitivity for central alterations may stabilize interpretation in a functional direction, delaying the emergence of an organic signal that a more sensitive test could have revealed earlier.
-
 Figure 4: Interference EMG of the masseter muscle. It represents the most widespread approach in current dental practice: a predominantly descriptive evaluation of muscle activity, useful for documenting functional patterns but lacking specific sensitivity to central or structural alterations.
Figure 4: Interference EMG of the masseter muscle. It represents the most widespread approach in current dental practice: a predominantly descriptive evaluation of muscle activity, useful for documenting functional patterns but lacking specific sensitivity to central or structural alterations. -
 Figure 5: Jaw jerk (masseter reflex). A higher diagnostic level, within neurology, allowing a first assessment of trigeminal reflex integrity. In the absence of further information, the picture may be interpreted as compatible with a functional disorder (TMD), without conclusive evidence of central pathology.
Figure 5: Jaw jerk (masseter reflex). A higher diagnostic level, within neurology, allowing a first assessment of trigeminal reflex integrity. In the absence of further information, the picture may be interpreted as compatible with a functional disorder (TMD), without conclusive evidence of central pathology. -
 Figure 6: Integrated Root-MEPs → jaw jerk sequence. When trigeminal Root-MEPs precede the jaw jerk, a marked amplitude asymmetry emerges, indicative of a central structural alteration. In this context, the subsequent reflex evaluation acquires a different clinical meaning, guiding the diagnostic pathway toward neuroradiological investigations, which in this case documented a structural brain lesion on MRI.
Figure 6: Integrated Root-MEPs → jaw jerk sequence. When trigeminal Root-MEPs precede the jaw jerk, a marked amplitude asymmetry emerges, indicative of a central structural alteration. In this context, the subsequent reflex evaluation acquires a different clinical meaning, guiding the diagnostic pathway toward neuroradiological investigations, which in this case documented a structural brain lesion on MRI.



This phenomenon is not a mathematical artifact, but a compact description of a real clinical experience.
From classical Bayes to quantum-like Bayes
In the described context, total probability can no longer be interpreted as a simple sum of independent contributions. When multiple diagnostic hypotheses share similar clinical signs, they enter informational competition.
To describe this dynamics, the classical Bayesian formalism can be extended by introducing an interference term:
The term does not represent a physical angle, but a measure of clinical overlap between alternative diagnostic hypotheses. When two conditions produce similar symptoms, interference reduces diagnostic certainty—not because of error, but because of an excess of competing information.[6][7][8]
Why a state index is needed
The results presented indicate that diagnosis cannot be reduced to a single scalar numerical value. What matters is not only the magnitude of an index, but the overall configuration of the clinical state: magnitude, phase, orientation, and dependence on the observational path.
It is within this context that the need arises for a mesoscopic vector index, capable of representing the system’s clinical state in a way that cannot be reduced to the binary classification healthy/sick.-
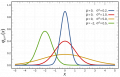 Figure 7: Classical scalar model and probability distribution. In the traditional diagnostic model, clinical information is represented as a numerical value along a one-dimensional line. The bell-shaped distribution does not introduce a new descriptive dimension of the clinical state, but expresses only the frequency of occurrence of the value along the same variable.
Figure 7: Classical scalar model and probability distribution. In the traditional diagnostic model, clinical information is represented as a numerical value along a one-dimensional line. The bell-shaped distribution does not introduce a new descriptive dimension of the clinical state, but expresses only the frequency of occurrence of the value along the same variable. -
 Figure 8: Vector representation of the clinical state (magnitude and phase). In the vector model, the system’s clinical state is no longer described by a single scalar value, but by a vector in informational space. Magnitude represents the intensity or degree of symmetry of the observed phenomenon, while phase encodes the relational configuration and the informational orientation of the system.
Figure 8: Vector representation of the clinical state (magnitude and phase). In the vector model, the system’s clinical state is no longer described by a single scalar value, but by a vector in informational space. Magnitude represents the intensity or degree of symmetry of the observed phenomenon, while phase encodes the relational configuration and the informational orientation of the system.


{kind=link}
Toward the Index
The Index is not conceived as a definitive diagnostic parameter, but as an indicator of the system’s informational configuration at a given time point.
Its function is to make explicit a verifiable epistemological fracture:
the assumption of commutativity of clinical information is not always valid.
Within this framework, the adoption of a quantum-like formalism does not stem from a mathematical analogy, but from the need to describe clinical systems that are non-commutative, dependent on observational order, and characterized by informational superposition.It is important to note that the 'Ψ Index', introduced in this chapter as a scalar clinical quantity, already contains in nuce the possibility of a vector formalization. From this perspective, it can be represented as a state vector |Ψ⟩, in order to make explicit its non-scalar, non-commutative nature and its dependence on the observational context.
Artificial intelligence is therefore introduced not as a tool for diagnostic automation, but as an operator of semantic and inferential decryption, capable of integrating heterogeneous signals, clinical narrative, and neurophysiological data into a coherent state configuration.
In the following chapters, these elements will be developed operationally, leading to the construction of the |Ψ⟩ Index as a dimensionless, normalized, and vectorial clinical state index, capable of representing not only the intensity of observed phenomena, but also their relational structure and their informational order.
Note how, already at this stage, the 'Ψ Index' has transformed into the '|Ψ⟩ Index'. This transformation describes how a scalar value can be formalized as a state vector |Ψ⟩, in order to make explicit its non-scalar, non-commutative nature and its dependence on the observational context.
- ↑ Ahmed Yaseen Alqutaibi, Maged S Alhammadi, Hatem Hazzaa Hamadallah, Ammar Abdulrahman Altarjami, Omar Talal Malosh 4, Aseel Mohammed Aloufi 4, Lama Mohammed Alkahtani, Faten Safran Alharbi 4, Esam Halboub, Abeer A Almashraqi. Global prevalence of temporomandibular disorders: a systematic review and meta-analysis. J Oral Facial Pain Headache. 2025 Jun;39(2):48-65. doi: 10.22514/jofph.2025.025. Epub 2025 Jun 12.PMID: 41070533
- ↑ Suga T, Uehara O, Abiko Y, Toyofuku A. Evaluating Large Language Models for Burning Mouth Syndrome Diagnosis. J Pain Res. 2025 Mar 19;18:1387-1405. doi: 10.2147/JPR.S509845. eCollection 2025.PMID: 40124539
- ↑ Knezevic MJ, Knezevic A, Boban J, Maletin A, Milekic B, Koprivica DD, Puskar T, Semnic R.. High-Field Magnetic Resonance Imaging of the Temporomandibular Joint Low Agreement with Clinical Diagnosis in Asymptomatic Females. Diagnostics (Basel). 2023 Jun 6;13(12):1986. doi: 10.3390/diagnostics13121986.PMID: 37370881
- ↑ Bianchi J, Roberto Gonçalves J, Carlos de Oliveira Ruellas A, Vieira Pastana Bianchi J, Ashman LM, Yatabe M, Benavides E, Soki FN, Cevidanes LHS.. Radiographic interpretation using high-resolution Cbct to diagnose degenerative temporomandibular joint disease. PLoS One. 2021 Aug 10;16(8):e0255937. doi: 10.1371/journal.pone.0255937. eCollection 2021.PMID: 34375354
- ↑ Dąbkowska I, Sobiech L, Czępińska A, Bęben A, Turżańska K, Gawda P. Multimodal Approaches in the Management of Temporomandibular Disorders: A Narrative Review. J Clin Med. 2025 Jun 17;14(12):4326. doi: 10.3390/jcm14124326.PMID: 40566071
- ↑ Asano M., Khrennikov A., Ohya M., Tanaka Y., Yamato I. Quantum Adaptivity in Biology: From Genetics To Cognition Springer, Heidelberg-Berlin-New York(2015)
- ↑ Busemeyer J., Bruza P. Quantum Models of Cognition and Decision Cambridge Univ. Press, Cambridge(2012)
- ↑ Basieva I, Khrennikov A, Ozawa M. Quantum-like modeling in biology with open quantum systems and instruments.Biosystems. 2021 Mar;201:104328. doi: 10.1016/j.biosystems.2020.104328. Epub 2020 Dec 24.PMID: 33347968