2° Clinical case: Pineal Cavernoma Abstract
2° Clinical case: Pineal Cavernoma
 |
Abstract
This chapter presents a complex clinical case of a 32-year-old male patient affected by severe nocturnal and diurnal bruxism associated with chronic bilateral orofacial pain, predominantly on the left side, and a progressive constellation of neurological signs. Unlike conventional interpretations that frame bruxism primarily as a dental parafunction or an occlusal disorder, the present work deliberately adopts a neurophysiological and systems-oriented perspective. The clinical history spans over 15 years of standard dental management, including prolonged use of occlusal bite planes, without meaningful symptom resolution, ultimately leading to diagnostic reconsideration.
The case is analyzed through a dual-context framework, distinguishing between the dental context and the neurological context, in order to address the frequent diagnostic overlap between temporomandibular disorders, primary headaches, dystonic phenomena, and disorders of central nervous system excitability. The chapter introduces dystonia, and in particular cranial and orofacial dystonia, as a conceptual bridge linking bruxism, orofacial pain, and abnormal neuromotor control. Special attention is given to the role of trigeminal motor and sensory systems, as well as to the modulation of mandibular reflexes under pain conditions.
Clinically, the patient exhibited not only persistent bruxism and orofacial pain, but also progressive neurological signs including jaw stiffness, diplopia, nystagmus, blurred optic disc margins, bilateral Babinski signs, polykinetic tendon reflexes, and trunk and limb muscle rigidity. This multisystem involvement challenged any purely dental interpretation. Electrophysiological investigations—including electromyography, motor evoked potentials of the trigeminal roots, jaw jerk testing, and evaluation of silent periods—revealed subtle but clinically relevant abnormalities, suggesting altered reflex excitability and central modulation rather than structural temporomandibular pathology.
To resolve apparent contradictions between normal dental findings and equivocal neurological signs, the chapter applies a formal logical diagnostic model previously introduced in Masticationpedia. Central to this model is the “demarcator of diagnostic coherence” (τ), a weighting parameter that assigns clinical significance based not only on the presence or absence of abnormalities, but on their intrinsic severity within a given context. Through this approach, low-weight normative dental data are filtered out, while even modest neurophysiological abnormalities acquire decisive diagnostic relevance. In the present case, the application of τ produces a diagnostic slope favoring a neurological interpretation, despite the absence of gross structural lesions.
The chapter argues that bruxism, in this context, should be interpreted as a possible macroscopic manifestation of neuromotor hyperexcitability rather than as a primary dental disorder. The concept of “machine language” of the central nervous system is introduced to describe how mesoscopic neurophysiological alterations—such as reflex facilitation, altered inhibitory control, and trigeminal system sensitization—may be translated into nonspecific clinical labels like bruxism. This reframing has significant implications for diagnosis, treatment, and interdisciplinary collaboration.
The chapter concludes by positioning this case as a paradigmatic example of the limitations of traditional diagnostic silos. It proposes a neurophysiological roadmap for further investigation, setting the stage for the subsequent chapter, “Encrypted Code: Hyperexcitability of the Trigeminal System,” in which the underlying mechanisms of central excitability and reflex modulation will be explored in greater depth.
-
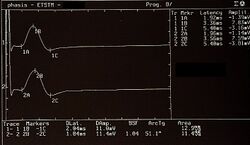 Figure 5: Motor Evoked Potentials of the trigeminal roots
Figure 5: Motor Evoked Potentials of the trigeminal roots -
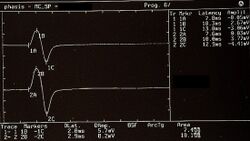 Figure 6: Jaw jerk detected electrophysiologically on the right (upper traces) and left (lower traces) masseters. The morphology and duration of the silent periods called 'Esteroceptive Suppression' appear to be symmetrical.
Figure 6: Jaw jerk detected electrophysiologically on the right (upper traces) and left (lower traces) masseters. The morphology and duration of the silent periods called 'Esteroceptive Suppression' appear to be symmetrical. -
 Figure 7: Electrical silent period detected electrophysiologically on the right (upper superimposed traces) and left (lower superimposed traces) masseters
Figure 7: Electrical silent period detected electrophysiologically on the right (upper superimposed traces) and left (lower superimposed traces) masseters



{kind=link}
🧠 Three guiding questions (with essential answers)
1️⃣ Why can severe bruxism no longer be interpreted exclusively as a dental or occlusal disorder? — Because long-term clinical observation and neurophysiological testing show that bruxism may persist despite normal occlusal findings and adequate dental treatment, indicating that it can represent a manifestation of central neuromotor hyperexcitability rather than a primary peripheral dental pathology.
2️⃣ Why is a neurophysiological approach essential in complex bruxism cases with orofacial pain? — Because electrophysiological investigations of trigeminal reflexes, motor evoked potentials, and muscle activity can reveal subtle abnormalities in central modulation and reflex excitability that are invisible to imaging or dental examinations but crucial for correct etiological attribution.
3️⃣ What is the diagnostic role of the coherence demarcator (τ) in this clinical model? — The demarcator τ assigns diagnostic weight based on the intrinsic clinical severity of findings, allowing low-impact normative data to be filtered out and enabling even mild but high-significance neurophysiological abnormalities to guide the diagnostic pathway toward the central nervous system.
If you already have an approved account, click on your profile icon and return to the Book Index to read the complete chapter.
To access the full content, you must sign in via LinkedIn and request approval.
Bibliography & references
- Thompson PD, Obeso JA, Delgado G, Gallego J, Marsden CD. Focal dystonia of the jaw and differential diagnosis of unilateral jaw and masticatory spasm. J Neurol Neurosurg Psychiatry. 1986;49:651–656. DOI: 10.1136/jnnp.49.6.651.
- Fernandes G, Franco AL, Gonçalves DA, Speciali JG, Bigal ME, Camparis CM. Temporomandibular disorders, sleep bruxism, and primary headaches are mutually associated. J Orofac Pain. 2013;27(1):14–20.
- Lobbezoo F. Taking up challenges at the interface of wear and tear. J Dent Res. 2007;86(2):101–103. DOI: 10.1177/154405910708600201.
- Dubner R, Ren K. Brainstem mechanisms of persistent pain following injury. J Orofac Pain. 2004;18(4):299–305.
- Wang K, Svensson P, Arendt-Nielsen L. Modulation of exteroceptive suppression periods in human jaw-closing muscles by experimental muscle pain. Pain. 1999;82(3):253–262. DOI: 10.1016/S0304-3959(99)00058-5.
- Ro JY, Capra NF. Modulation of jaw muscle spindle afferent activity following intramuscular injections with hypertonic saline. Pain. 2001;92(1–2):117–127.
- Winocur E, Gavish A, Voikovitch M, Emodi-Perlman A, Eli I. Drugs and bruxism: a critical review. J Orofac Pain. 2003;17(2):99–111.
- Katsarava Z, Egelhof T, Kaube H, Diener HC, Limmroth V. Symptomatic migraine and sensitization of trigeminal nociception associated with contralateral pontine cavernoma. Pain. 2003;105(1–2):381–384.
- Watanabe S, Mochizuki H, Nakashima I, Itoyama Y. Primary Sjögren's syndrome with CNS disease mimicking chronic progressive multiple sclerosis. Rinsho Shinkeigaku. 1998;38(7):658–662.
- Norlinah MI, Bhatia KP, Ostergaard K, Howard R, Arabia G, Quinn NP. Primary lateral sclerosis mimicking atypical parkinsonism. Mov Disord. 2007;22(14):2057–2062. DOI: 10.1002/mds.21645.
- Yoshida M, Murakami N, Hashizume Y, Takahashi A. Motor neuron disease with dementia: clinicopathological study. Rinsho Shinkeigaku. 1992;32(11):1193–1202.
- Cruccu G, Inghilleri M, Fraioli B, Guidetti B. Neurophysiologic assessment of trigeminal function after surgery for trigeminal neuralgia. Neurology. 1987;37:631–638.
- Kaufman MD. Masticatory spasm in facial hemiatrophy. Ann Neurol. 1980;7:585–587.