The logic of the classical language Abstract: differenze tra le versioni
Nessun oggetto della modifica |
Nessun oggetto della modifica |
||
| Riga 7: | Riga 7: | ||
|no title=1 | |no title=1 | ||
}} | }} | ||
{{ArtBy| | {{ArtBy| | ||
| autore = Gianni Frisardi | | autore = Gianni Frisardi | ||
| Riga 12: | Riga 13: | ||
| autore3 = Flavio Frisardi | | autore3 = Flavio Frisardi | ||
}} | }} | ||
<div class="chapter-content"> | <div class="chapter-content"> | ||
== Abstract == | == Abstract == | ||
This chapter introduces the '''logic of classical language''' as a conceptual tool for understanding how medicine constructs “certain” diagnoses from signs, symptoms, and instrumental data. The goal is not to deny the effectiveness of traditional semiotics, but to show that clinical language—even when it appears rigorous—remains anchored to '''interpretive contexts''' that may generate divergent conclusions without any change in biological reality. | |||
The chapter revisits the clinical case of '''Mary Poppins''', already discussed in the introductory chapter on the logic of medical language and on the concept of an encrypted “machine message.” Here, however, the same problem is approached differently: we observe how the classical approach tends to transform clinical observation into a system of “if… then” propositions, supported by the law of the '''excluded middle''' (true/false) and by proof by contradiction. In other words, classical logic naturally pushes toward a dichotomous diagnosis: “TMD yes / TMD no.” | |||
To make the mechanism transparent, the chapter builds a formal framework based on '''propositions and predicates''', where instrumental evidence (CT, stratigraphy, axiography, EMG pattern) becomes the premise <math>A(x)</math>, and the diagnosis of temporomandibular disorder becomes the consequence <math>B(x)</math>. If Mary Poppins is included in the set of “normal patients” within the dental context, the deduction is coherent: <math>A(a)\rightarrow B(a)</math>. Here the strength of classical logic appears as an advantage: it enables internal coherence, local validation, and the construction of protocols. | |||
The difficulty arises when another specialist—e.g., the neurologist—proposes an alternative interpretation: Mary Poppins may not belong to the set <math>x</math> of “normal patients” for dentistry, and therefore the deductive rule would not apply. From this mismatch emerges the most important theme of the chapter: a diagnosis can be '''logically correct''' within a context and yet '''not clinically exhaustive''' in a broader context. For this reason, the chapter introduces the concepts of '''logical compatibility and incompatibility''' between sets of assertions (<math>\Im</math>, <math>\delta_1...\delta_n</math>): internal coherence can grow indefinitely without guaranteeing universality. | |||
The chapter concludes by suggesting that classical logic, although indispensable, shows structural limits when it encounters complex biological systems and early, non-observable phenomena. The need to move beyond “black or white” prepares the transition toward more flexible logics, especially probabilistic logic. | |||
==2nd Clinical Approach== | == 2nd Clinical Approach == | ||
(Hover over the images) | (Hover over the images) | ||
<center> | |||
<gallery widths="350" heights="282" perrow="2" mode="slideshow"> | <gallery widths="350" heights="282" perrow="2" mode="slideshow"> | ||
File:Spasmo emimasticatorio.jpg|Figure 2: Patient reports "orofacial pain" on the right facial hemisphere. | File:Spasmo emimasticatorio.jpg|Figure 2: Patient reports "orofacial pain" on the right facial hemisphere. | ||
| Riga 34: | Riga 38: | ||
File:Spasmo emimasticatorio assiografia.jpg|Figure 5: Axiography of the patient showing a flattening of the masticatory pattern at the level of the right condyle. | File:Spasmo emimasticatorio assiografia.jpg|Figure 5: Axiography of the patient showing a flattening of the masticatory pattern at the level of the right condyle. | ||
File:EMG2.jpg|Figure 6: Interfering EMG activity. Overlapping upper traces corresponding to the right masseter, below to the left masseter. | File:EMG2.jpg|Figure 6: Interfering EMG activity. Overlapping upper traces corresponding to the right masseter, below to the left masseter. | ||
</gallery></center> | </gallery> | ||
</center> | |||
=== Three guiding questions (with short answers) === | |||
🔴 '''Why is medical language structurally fragile, even when it seems rigorous?'''<br> | |||
Because it is a hybrid language: it borrows words from everyday speech, but assigns them technical meanings that vary across disciplines. The same “sign” can therefore be interpreted through different clinical grammars. | |||
🟡 '''Why can one clinical case generate conflicting diagnoses without any change in the facts?'''<br> | |||
Because classical reasoning often depends on the reference set being used (“normal patients” for dentistry vs. “atypical patients” for neurology). The logic may be coherent inside each context, yet the contexts are not equivalent. | |||
🔵 '''How can classical logic be internally correct and still be clinically incomplete?'''<br> | |||
Because internal coherence can be expanded indefinitely by adding compatible assertions (<math>\delta_1...\delta_n</math>) without guaranteeing that the same conclusion remains valid outside the original domain. Complex systems can require broader—and probabilistic—interpretive frameworks. | |||
<div style="border:1px solid #d8d8d8; border-radius:14px; padding:18px 20px; background:#fafafa; margin:22px 0;"> | <div style="border:1px solid #d8d8d8; border-radius:14px; padding:18px 20px; background:#fafafa; margin:22px 0;"> | ||
| Riga 52: | Riga 68: | ||
</div> | </div> | ||
</html> | </html> | ||
<onlyinclude> | <onlyinclude> | ||
| Riga 122: | Riga 137: | ||
* {{cite book | autore = LeResche L | titolo = Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors | url = https://pubmed.ncbi.nlm.nih.gov/9260045/ | opera = Crit Rev Oral Biol Med | anno = 1997 | PMID = 9260045 | DOI = 10.1177/10454411970080030401 }} | * {{cite book | autore = LeResche L | titolo = Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors | url = https://pubmed.ncbi.nlm.nih.gov/9260045/ | opera = Crit Rev Oral Biol Med | anno = 1997 | PMID = 9260045 | DOI = 10.1177/10454411970080030401 }} | ||
</onlyinclude> | </onlyinclude> | ||
</div> | </div> | ||
Versione delle 18:03, 29 dic 2025
 |
Abstract
This chapter introduces the logic of classical language as a conceptual tool for understanding how medicine constructs “certain” diagnoses from signs, symptoms, and instrumental data. The goal is not to deny the effectiveness of traditional semiotics, but to show that clinical language—even when it appears rigorous—remains anchored to interpretive contexts that may generate divergent conclusions without any change in biological reality.
The chapter revisits the clinical case of Mary Poppins, already discussed in the introductory chapter on the logic of medical language and on the concept of an encrypted “machine message.” Here, however, the same problem is approached differently: we observe how the classical approach tends to transform clinical observation into a system of “if… then” propositions, supported by the law of the excluded middle (true/false) and by proof by contradiction. In other words, classical logic naturally pushes toward a dichotomous diagnosis: “TMD yes / TMD no.”
To make the mechanism transparent, the chapter builds a formal framework based on propositions and predicates, where instrumental evidence (CT, stratigraphy, axiography, EMG pattern) becomes the premise , and the diagnosis of temporomandibular disorder becomes the consequence . If Mary Poppins is included in the set of “normal patients” within the dental context, the deduction is coherent: . Here the strength of classical logic appears as an advantage: it enables internal coherence, local validation, and the construction of protocols.
The difficulty arises when another specialist—e.g., the neurologist—proposes an alternative interpretation: Mary Poppins may not belong to the set of “normal patients” for dentistry, and therefore the deductive rule would not apply. From this mismatch emerges the most important theme of the chapter: a diagnosis can be logically correct within a context and yet not clinically exhaustive in a broader context. For this reason, the chapter introduces the concepts of logical compatibility and incompatibility between sets of assertions (, ): internal coherence can grow indefinitely without guaranteeing universality.
The chapter concludes by suggesting that classical logic, although indispensable, shows structural limits when it encounters complex biological systems and early, non-observable phenomena. The need to move beyond “black or white” prepares the transition toward more flexible logics, especially probabilistic logic.
2nd Clinical Approach
(Hover over the images)
-
 Figure 2: Patient reports "orofacial pain" on the right facial hemisphere.
Figure 2: Patient reports "orofacial pain" on the right facial hemisphere. -
 Figure 3: Stratigraphy of the temporomandibular joint (TMJ) of the patient showing signs of condylar flattening and presence of osteophytes.
Figure 3: Stratigraphy of the temporomandibular joint (TMJ) of the patient showing signs of condylar flattening and presence of osteophytes. -
 Figure 4: Computed tomography of the TMJ
Figure 4: Computed tomography of the TMJ -
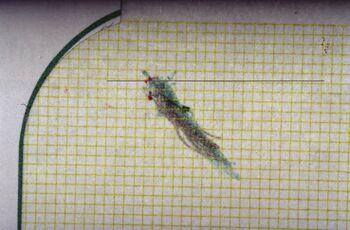 Figure 5: Axiography of the patient showing a flattening of the masticatory pattern at the level of the right condyle.
Figure 5: Axiography of the patient showing a flattening of the masticatory pattern at the level of the right condyle. -
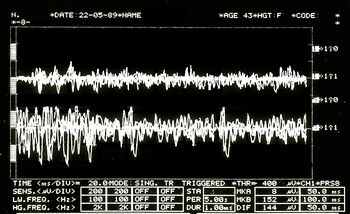 Figure 6: Interfering EMG activity. Overlapping upper traces corresponding to the right masseter, below to the left masseter.
Figure 6: Interfering EMG activity. Overlapping upper traces corresponding to the right masseter, below to the left masseter.





Three guiding questions (with short answers)
🔴 Why is medical language structurally fragile, even when it seems rigorous?
Because it is a hybrid language: it borrows words from everyday speech, but assigns them technical meanings that vary across disciplines. The same “sign” can therefore be interpreted through different clinical grammars.
🟡 Why can one clinical case generate conflicting diagnoses without any change in the facts?
Because classical reasoning often depends on the reference set being used (“normal patients” for dentistry vs. “atypical patients” for neurology). The logic may be coherent inside each context, yet the contexts are not equivalent.
🔵 How can classical logic be internally correct and still be clinically incomplete?
Because internal coherence can be expanded indefinitely by adding compatible assertions () without guaranteeing that the same conclusion remains valid outside the original domain. Complex systems can require broader—and probabilistic—interpretive frameworks.
🔒 Access to the full chapter
👤 Approved users — click on your profile icon and return to the Book Index to read the complete chapter.
🔑 New readers — sign in via LinkedIn to request access.
- Stanley DE, Campos DG, «The logic of medical diagnosis», in Perspect Biol Med, 2013».
PMID:23974509
DOI:10.1353/pbm.2013.0019
- Croskerry P, «Adaptive expertise in medical decision making», in Med Teach, 2018».
PMID:30033794
DOI:10.1080/0142159X.2018.1484898
- Townsend GC, Brook AH, «The face, the future, and dental practice: how research in craniofacial biology will influence patient care», in Aust Dent J, Australian Dental Association, 2014».
PMID:24646132
DOI:10.1111/adj.12157
- Sperber GH, Sperber SM, «The genesis of craniofacial biology as a health science discipline», in Aust Dent J, Australian Dental Association, 2014».
PMID:24495071
DOI:10.1111/adj.12131
- Brook AH, Brook O'Donnell M, Hone A, Hart E, Hughes TE, Smith RN, Townsend GC, «General and craniofacial development are complex adaptive processes influenced by diversity», in Aust Dent J, Australian Dental Association, 2014».
PMID:24617813
DOI:10.1111/adj.12158
- Williams SD, Hughes TE, Adler CJ, Brook AH, Townsend GC, «Epigenetics: a new frontier in dentistry», in Aust Dent J, Australian Dental Association, 2014».
PMID:24611746
DOI:10.1111/adj.12155
- Yong R, Ranjitkar S, Townsend GC, Brook AH, Smith RN, Evans AR, Hughes TE, Lekkas D, «Dental phenomics: advancing genotype to phenotype correlations in craniofacial research», in Aust Dent J, Australian Dental Association, 2014».
PMID:24611797
DOI:10.1111/adj.12156
- Thesleff I, «Current understanding of the process of tooth formation: transfer from the laboratory to the clinic», in Aust Dent J, 2013».
DOI:10.1111/adj.12102
- Peterkova R, Hovorakova M, Peterka M, Lesot H, «Three-dimensional analysis of the early development of the dentition», in Aust Dent J, Wiley Publishing Asia Pty Ltd on behalf of Australian Dental Association, 2014».
DOI:10.1111/adj.12130
- Lesot H, Hovorakova M, Peterka M, Peterkova R, «Three-dimensional analysis of molar development in the mouse from the cap to bell stage», in Aust Dent J, 2014».
DOI:10.1111/adj.12132
- Hughes TE, Townsend GC, Pinkerton SK, Bockmann MR, Seow WK, Brook AH, Richards LC, Mihailidis S, Ranjitkar S, Lekkas D, «The teeth and faces of twins: providing insights into dentofacial development and oral health for practising oral health professionals», in Aust Dent J, 2013».
DOI:10.1111/adj.12101
- Han J, Menicanin D, Gronthos S, Bartold PM, «Stem cells, tissue engineering and periodontal regeneration», in Aust Dent J, 2013».
DOI:10.1111/adj.12100
- Brook AH, Jernvall J, Smith RN, Hughes TE, Townsend GC, «The Dentition: The Outcomes of Morphogenesis Leading to Variations of Tooth Number, Size and Shape», in Aust Dent J, 2014».
DOI:10.1111/adj.12160
- Seow WK, «Developmental defects of enamel and dentine: challenges for basic science research and clinical management», in Aust Dent J, 2014».
PMID:24164394
DOI:10.1111/adj.12104
- Kieser JA, Farland MG, Jack H, Farella M, Wang Y, Rohrle O, «The role of oral soft tissues in swallowing function: what can tongue pressure tell us?», in Aust Dent J, 2013».
DOI:10.1111/adj.12103
- Slavkin HC, «Research on Craniofacial Genetics and Developmental Biology: Implications for the Future of Academic Dentistry», in J Dent Educ, 1983».
PMID:6573384
- Slavkin HC, «The Future of Research in Craniofacial Biology and What This Will Mean for Oral Health Professional Education and Clinical Practice», in Aust Dent J, 2014».
PMID:24433547
DOI:10.1111/adj.12105
- Littlewood SJ, Kandasamy S, Huang G, «Retention and relapse in clinical practice», in Aust Dent J, 2017».
DOI:10.1111/adj.12475
- Miamoto CB, Silva Marques L, Abreu LG, Paiva SM, «Impact of two early treatment protocols for anterior dental crossbite on children’s quality of life», in Dental Press J Orthod, 2018».
- Alachioti XS, Dimopoulou E, Vlasakidou A, Athanasiou AE, «Amelogenesis imperfecta and anterior open bite: Etiological, classification, clinical and management interrelationships», in J Orthod Sci, 2014».
DOI:10.4103/2278-0203.127547
- Mizrahi E, «A review of anterior open bite», in Br J Orthod, 1978».
PMID:284793
DOI:10.1179/bjo.5.1.21
- Pereira LM, Pinto AM, «Reductio ad Absurdum Argumentation in Normal Logic Programs», Arg NMR, 2007, Tempe, Arizona - Caparica, Portugal – in «Argumentation and Non-Monotonic Reasoning - An LPNMR Workshop».
- Castroflorio T, Talpone F, Deregibus A, Piancino MG, Bracco P, «Effects of a Functional Appliance on Masticatory Muscles of Young Adults Suffering From Muscle-Related Temporomandibular Disorder», in J Oral Rehabil, 2004».
PMID:15189308
DOI:10.1111/j.1365-2842.2004.01274.x
- Maeda N, Kodama N, Manda Y, Kawakami S, Oki K, Minagi S, «Characteristics of Grouped Discharge Waveforms Observed in Long-term Masseter Muscle Electromyographic Recording: A Preliminary Study», in Acta Med Okayama, 2019».
PMID:31439959
DOI:10.18926/AMO/56938
- Rudy TE, «Psychophysiological Assessment in Chronic Orofacial Pain», in Anesth Prog, 1990».
PMID:2085203 - PMCID:PMC2190318
- Woźniak K, Piątkowska D, Lipski M, Mehr K, «Surface electromyography in orthodontics - a literature review», in Med Sci Monit, 2013».
PMID:23722255 - PMCID:PMC3673808
DOI:10.12659/MSM.883927
- Liang X, Liu S, Qu X, Wang Z, Zheng J, Xie X, Ma G, Zhang Z, Ma X, «Evaluation of Trabecular Structure Changes in Osteoarthritis of the Temporomandibular Joint With Cone Beam Computed Tomography Imaging», in Oral Surg Oral Med Oral Pathol Oral Radiol, 2017».
PMID:28732700
DOI:10.1016/j.oooo.2017.05.514
- Solberg WK, Bibb CA, Nordström BB, Hansson TL, «Malocclusion Associated With Temporomandibular Joint Changes in Young Adults at Autopsy», in Am J Orthod, 1986».
PMID:3457531
DOI:10.1016/0002-9416(86)90055-2
- Kobs G, Didziulyte A, Kirlys R, Stacevicius M, «Reliability of ARCUSdigma (KaVo) in Diagnosing Temporomandibular Joint Pathology», in Stomatologija, 2007».
PMID:17637527
- Piancino MG, Roberi L, Frongia G, Reverdito M, Slavicek R, Bracco P, «Computerized axiography in TMD patients before and after therapy with 'function generating bites'», in J Oral Rehabil, 2008».
PMID:18197841
DOI:10.1111/j.1365-2842.2007.01815.x
- López-Cedrún J, Santana-Mora U, Pombo M, Pérez Del Palomar A, Alonso De la Peña V, Mora MJ, Santana U, «Jaw Biodynamic Data for 24 Patients With Chronic Unilateral Temporomandibular Disorder», in Sci Data, 2017».
PMID:29112190 - PMCID:PMC5674825
DOI:10.1038/sdata.2017.168
- Oliveira Mazzetto M, Almeida Rodrigues C, Valencise Magri L, Oliveira Melchior M, Paiva G, «Severity of TMD Related to Age, Sex and Electromyographic Analysis», in Braz Dent J, 2014».
DOI:10.1590/0103-6440201302310
- LeResche L, «Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors», in Crit Rev Oral Biol Med, 1997».
PMID:9260045
DOI:10.1177/10454411970080030401